



Two of the most common ailments are peripheral arterial disease and chronic venous insufficiency. Millions of people worldwide live with these diseases.
Both diseases involve the blood vessels. But: do you know the key differences between PAD and CVI?
This post discusses signs, symptoms, and treatment options for both PAD and CVI. This is a great place to start educating yourself on these vein issues.
However, if you suspect you have arterial or venous insufficiency, talk to your healthcare provider. You’ll want to take control of your health before either PAD or CVI worsens.
What is Peripheral Arterial Disease?
Patients with peripheral arterial disease, or PAD, have poor circulation in their lower legs. Plaque restricts blood flow, causing pain in the calf or thigh. This pain can make walking difficult.
Peripheral arterial disease is most commonly caused by fatty material in the arteries. Less common causes include injuries, radiation, or blood vessel inflammation(2).
PAD affects more than 200 million adults worldwide(1). Some risk factors for PAD include(3):
- Ethnicity
- Diabetes
- Obesity
- Smoking
- Hypertension
- Increased age
- Family history of PAD, heart disease, or stroke
- High blood levels of homocysteine
- High cholesterol levels
How Does Peripheral Arterial Disease Occur?
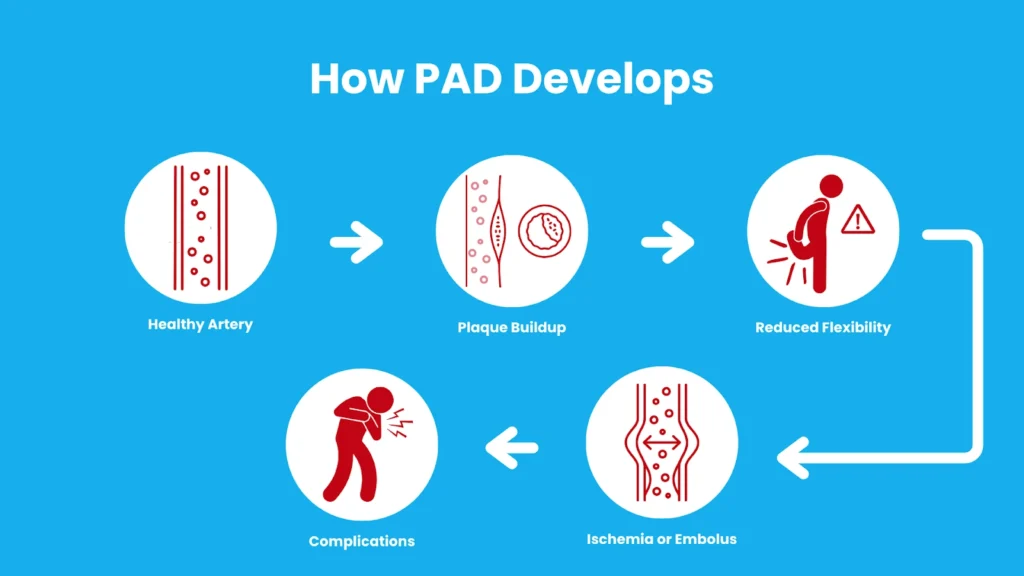
Peripheral arterial disease occurs when plaque slowly builds up inside the arteries and sticks to the walls(4).
In the early stages, arteries continue to function. Arteries stretch to maintain the flow. However, as this plaque increases, the arteries cease to stretch. At this point, the plaque restricts blood flow.
This can cause ischemia – a reduction or restriction of blood flow – in the lower leg. You might also experience an embolus, such as a blood clot.
When the artery is fully obstructed, blood flow can shift to smaller arteries. However, flow is limited due to their size.
Signs and Symptoms of Peripheral Arterial Disease

If you have PAD, you might experience pain in the lower legs that worsens while walking. Your legs may also feel crampy, heavy, or tired.
Patients with mild to moderate PAD may have little to no symptoms. This depends on where in the leg the PAD has occurred (if in a major artery or a minor one) or how active the patient is.
Patients with severe peripheral arterial disease may experience pain even while resting. These patients are often bed-bound. They may complain of burning pain, especially on the soles of the feet, and most often at night. This can lead to fatigue.
Patients with severe pain usually relieve their symptoms by dangling their legs. This can cause edema, however.
Other side effects include paleness, a decrease in muscle, hair loss, cool skin, or palpitations.
Peripheral Arterial Disease Diagnosis
To diagnose PAD, your doctor will perform a physical exam. They will take your blood pressure above your ankle and on both arms. (This is an ankle-brachial index, or ABI.)
They may order labs to check renal function and electrolyte levels. They may also perform Doppler exams to locate the site of the issue and its severity. They may order CT or MRA scans. An electrocardiogram (ECG/EKG) may be ordered to check for heart problems.
Treatments for Peripheral Arterial Disease
Patients with PAD should focus on lifestyle and mobility improvement. Doctors recommend a diet low in cholesterol and to avoid smoking. It is also important to manage certain conditions simultaneously, like diabetes or hypertension. This can help improve PAD symptoms(5).
Your doctor may also prescribe medications like cilostazol to improve circulation. Pentoxifylline may also be prescribed to increase oxygen delivery.
Consult with a medical professional before taking these medications. Certain comorbidities may contraindicate the intake of these medications.
Peripheral Arterial Disease Complications
Patients who do not make lifestyle changes are at risk of severe PAD. Peripheral arterial disease can progress to:
- Infections in the lower leg
- Ischemia or gangrene
- Stroke
- Blood clots
- Heart attack
- Erectile dysfunction
- Amputation
- Chronic venous insufficiency
And speaking of…
What is Chronic Venous Insufficiency (CVI)?
Chronic venous insufficiency is a disease that causes edema in the lower legs, skin changes, and discomfort. Many patients also have venous ulcers, which can be painful, and become infected.
Chronic venous insufficiency affects 7 million people in the United States(6).
CVI can either be primary or secondary to deep vein thrombosis:
Primary chronic venous insufficiency means that the symptoms occur without a prior disease.
Secondary chronic venous insufficiency occurs as a result of deep vein thrombosis. DVT triggers an inflammatory response.
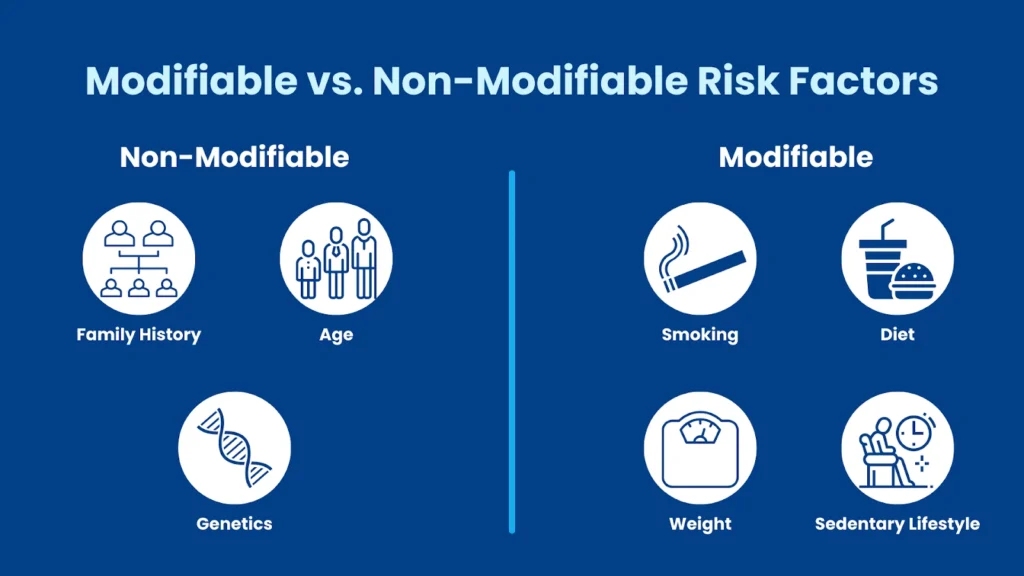
Modifiable risk factors of CVI include:
- Smoking
- Obesity
- Pregnancy
- Hypertension
- Hormonal birth control
- Prolonged standing
- Vein injury
- Deep vein thrombosis
Non-modifiable risk factors of CVI include being female or the May Thurner syndrome.
How Does Chronic Venous Insufficiency Occur?
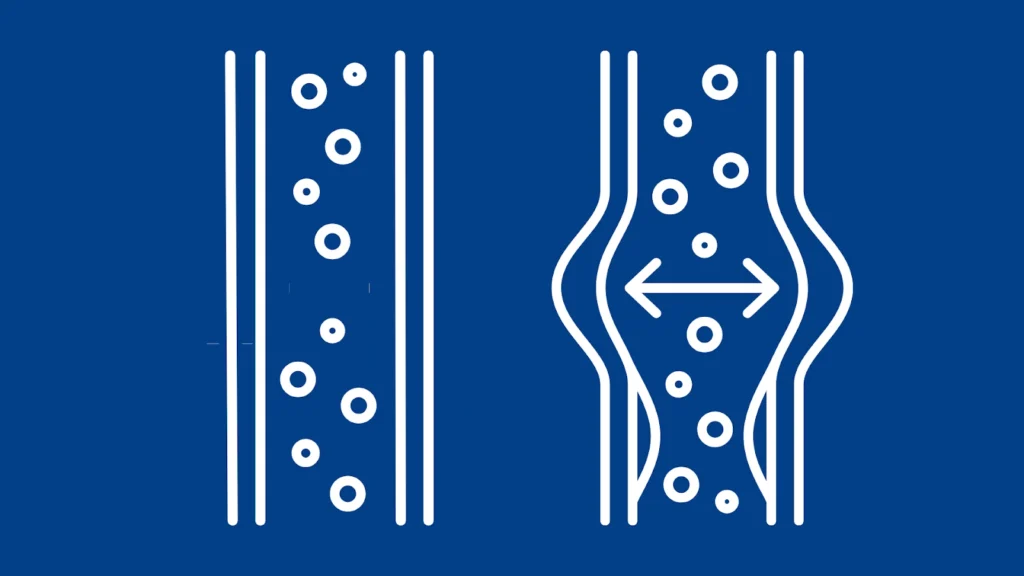
Chronic venous insufficiency occurs due to reflux or obstruction of venous blood flow. This backward flow stems from a weakened, expanded, or oddly shaped valve. In almost all cases, CVI leads to venous hypertension.
For some patients, this valve issue is genetic. For others, it may be due to thrombosis, trauma, prolonged standing, or hormonal changes.
Patients may experience pain, swelling, and even hyperpigmentation. They may also experience lipodermatosclerosis: when the skin thickens due to fat fibrosis. And, as the skin continues to weaken, ulcers may form.
Signs and Symptoms of Chronic Venous Insufficiency
Patients with CVI may experience lower leg swelling, discomfort, pain, fatigue, and itching. Some may complain of cramping or throbbing feeling relieved by resting or elevating their legs.
Unlike peripheral arterial disease, this pain is not associated with any activity.
As the disease worsens, varicose veins may develop in the legs. Patients may also experience lesions, ulcers, hyperpigmentation, and dermal atrophy.
Chronic Venous Insufficiency Diagnosis
To diagnose CVI, your doctor will review your medical history. It is important to share other conditions you may have. Take note of diseases that you have, especially diabetes and hypertension.
They will also perform a physical exam.
They may order a duplex ultrasonography to help identify affected regions. Invasive venography may be done in stenosis patients(7). The doctor may take an ankle-brachial index. This is to rule out other causes like peripheral arterial disease.
They may also order a blood test if the cause of the disease is unknown.
Treatment for Chronic Venous Insufficiency
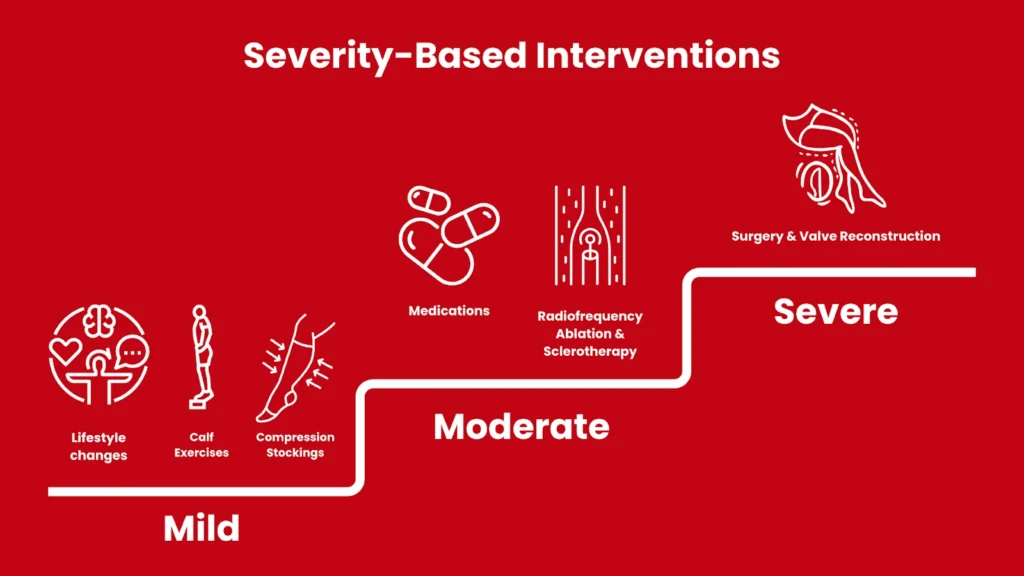
Patients with chronic venous insufficiency are treated based on disease severity.
Treatments for CVI aim to:
- Reduce leg discomfort or pain
- Reduce swelling
- Stabilize or improve leg appearance
- Remove painful varicose veins
- Heal ulcers and avoid infection
In early stages, patients may regularly elevate their legs, do calf exercises, and wear compression stockings.
Ulcers are treated with antibiotics and compression bandages. Compression bandages should be used with caution if PAD coexists. If ulcers do not heal, your doctor may recommend surgery.
Patients with superficial vein reflux may try radiofrequency ablation, vein stripping, or foam sclerotherapy.
Radiofrequency ablation, sclerotherapy, and subfascial endoscopic perforator surgery are recommended to treat perforator reflux.
Deep vein reflux is managed with a valve transplant or reconstruction.
Compression therapy is highly effective for managing CVI if a patient keeps at it.
Chronic Venous Insufficiency Complications
CVI complications include:
- Venous ulcers
- Thrombophlebitis
- Bleeding
- Chronic pain
- Secondary lymphedema
- Deep vein thrombosis
- Pulmonary embolism
Deep vein thrombosis and pulmonary embolism are emergency cases. These should be treated as soon as possible.
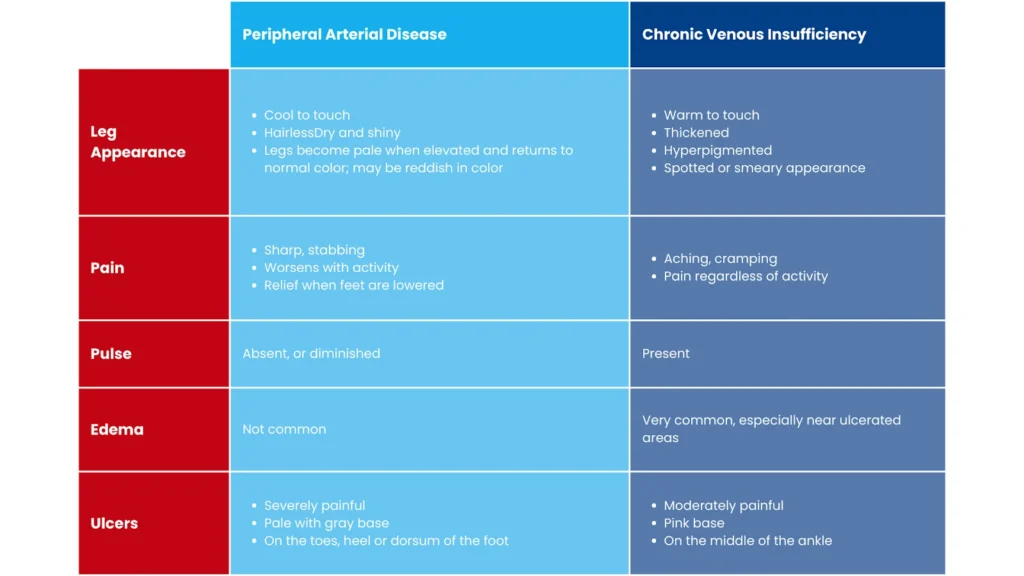
The Differences Between PAD and CVI
Peripheral arterial disease and chronic venous insufficiency may seem similar. However, there are key differences between these two diseases. We’ve summed up these differences in the chart below:
Conclusion
If you have any of the symptoms described in this post, don’t wait to get help. Whether it’s PAD, CVI, or a different vein disease, getting a proper diagnosis is the first step toward a healthier you and improving your quality of life.
Texas Vein Experts is here to provide solutions for PAD, CVI, and other vein diseases. Our team members are professional and patient-focused. We provide top-of-the-line care using the latest medical technology to provide treatment like radiofrequency ablation and sclerotherapy.
Don’t wait one day longer to get your vein health under control. Book your free consultation today!
References
- Zemaitis MR, Boll JM, Dreyer MA. Peripheral Arterial Disease. [Updated 2020 Jul 10]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2020 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK430745/
- Simon F, Oberhuber A, Floros N, Düppers P, Schelzig H, Duran M. Pathophysiology of chronic limb ischemia. Gefasschirurgie. 2018;23(Suppl 1):13-18.
- Jelani QU, Petrov M, Martinez SC, Holmvang L, Al-Shaibi K, Alasnag M. Peripheral Arterial Disease in Women: an Overview of Risk Factor Profile, Clinical Features, and Outcomes. Curr Atheroscler Rep. 2018 Jun 02;20(8):40
- Kim HO, Kim W. Elucidation of the Diagnosis and Treatment of Peripheral Arterial Disease. Korean Circ J. 2018 Sep;48(9):826-827.
- US Preventive Services Task Force. Curry SJ, Krist AH, Owens DK, Barry MJ, Caughey AB, Davidson KW, Doubeni CA, Epling JW, Kemper AR, Kubik M, Landefeld CS, Mangione CM, Silverstein M, Simon MA, Tseng CW, Wong JB. Screening for Peripheral Artery Disease and Cardiovascular Disease Risk Assessment With the Ankle-Brachial Index: US Preventive Services Task Force Recommendation Statement. JAMA. 2018 Jul 10;320(2):177-183.
- Patel SK, Surowiec SM. Venous Insufficiency. [Updated 2020 Aug 15]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2020 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK430975/
- Knupfer J, Reich-Schupke S, Stücker M. [Conservative management of varicosis and postthrombotic syndrome]. Hautarzt. 2018 May;69(5):413-424


